[smbtoolbar]
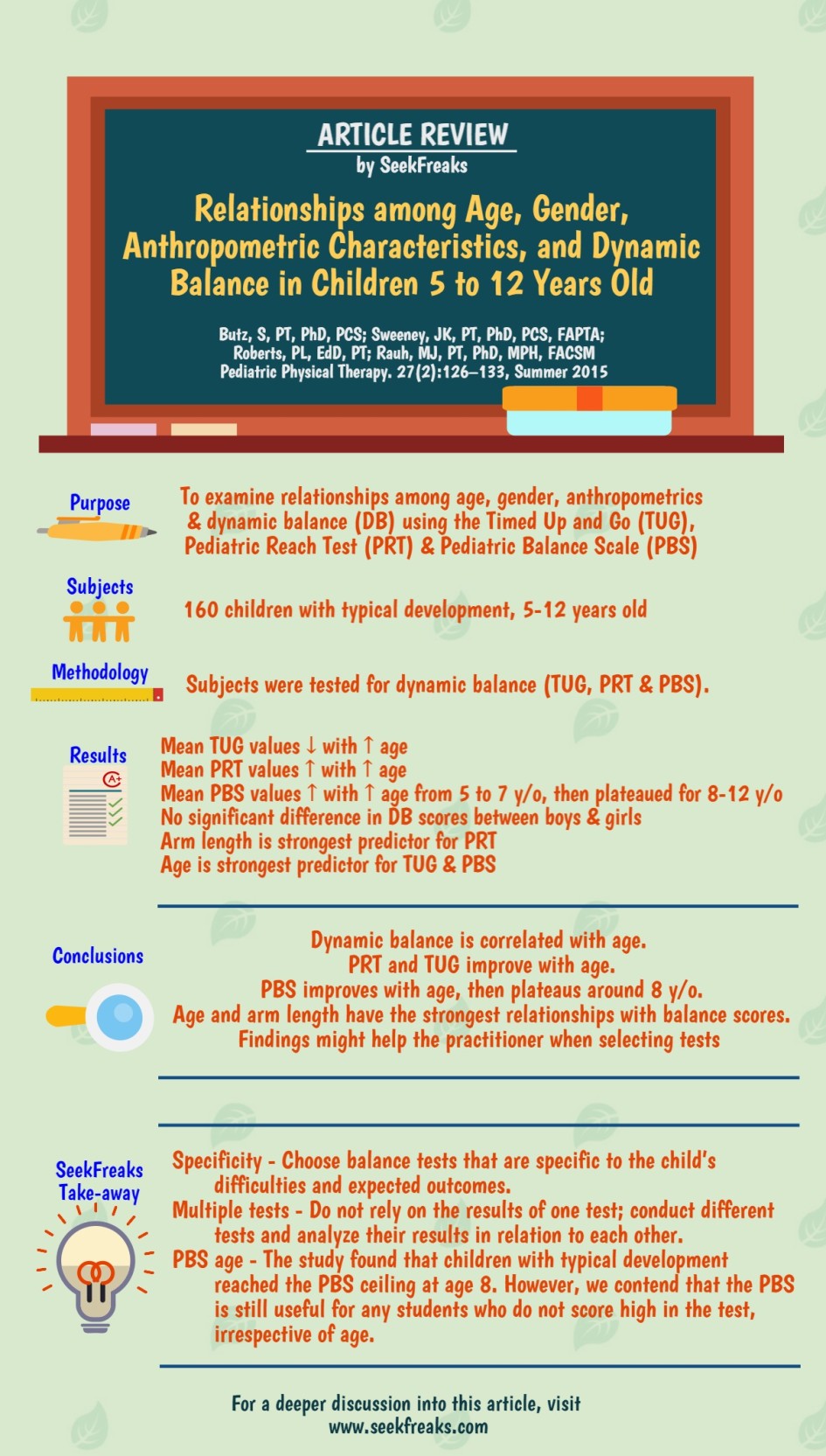
This article caught my eye since it is relevant to our recent post on the the 4 Pillars of PT Assessments. The investigators in this study wanted to determine whether dynamic balance is related to age, gender and anthropometrics measurements that include height, weight, arm length and foot length. Dynamic balance was measured using 3 different tests: the Timed Up and Go (TUG), Pediatric Reach Test (PRT) & Pediatric Balance Scale (PBS). Subjects included 160 girls and boys with typical development, 5-12 years old.
As expected, dynamic balance improves with age.
- On average, the TUG completion times shortened and the PRT measures increased from 5-12 years old.
- Although PBS improved from 5-7 years old, scores plateaued starting around 8 years old at the maximum score of 56. This is probably because the PBS uses an ordinal scoring with a ceiling, while the PRT and TUG does not have a definitive ceiling.
- The authors concluded that the PBS may not be as useful as the PRT and TUG for children 8 years or older. But, the PBS might be preferred for younger children since it contains more balance activities. Would this hold true in school-based PT practice?
Recall that the subjects in this study are children with typical development. On the other hand, the students we typically examine in the schools are students with disabilities who may not be reaching the PBS ceiling score of 56 at age 8 or even older. Therefore, for any student that is not reaching the highest scores of the PBS, irrespective of age, this test can still prove to be very useful. This is especially so, since the PBS has multiple functional components that can provide a variety of insights for the practitioner. Some of these are: retrieving object from the floor, reaching forward with outstretched hand, and transfers. That the PBS is able to rate these activities numerically makes it an excellent measurement of baseline dynamic balance and progress as a result of intervention.
The investigators in this study also found that arm length is the strongest predictor for the PRT, while height and foot length might be predictors as well. In the study’s Discussion, they cited correlations found by previous studies which included:
- one study found height as a stronger predictor of TUG scores for children 5-7 and 11-13 years old than age,
- another study found age is a strong predictor of the Functional Reach Test (FRT) for children 5-15 years old,
- one study found weight as a strong predictor of FRT for children 3-4 years old.
What do these seemingly contradictory findings mean for us?
These findings confirm that functional tasks have multiple contributing factors like body structures (mentioned in this study) or attributes such as strength, tone and flexibility (not included in this study). It is possible that their effects on function may differ from one individual or group of individuals to another. Various combinations of contributing factors (e.g., tall with weak leg muscles vs. short with weak leg muscles) may also affect function differently. Therefore, it is most advantageous to use more than one test when performing an examination. A single test alone may not provide you with a clear picture of the child’s abilities. Each of the tests in this study, for example, provides different insights:
- reaching ability from the PRT/FRT,
- transfers and a short walk with a 360 degree turn from the TUG,
- and various balance activities that does not include walking forward from the PBS.
Moreover, it is best to include observations (not just scores) when reporting test performance. Your description of the student’s body mechanics while performing these tests provide additional clues on the student’s specific strengths, weaknesses, preferred pattern, and compensation strategies. Thus, the use of multiple tests, together with descriptions of the child’s performance, provides you with a rich data set that will enhance your clinical judgment. This is true not just for testing balance but also for testing other aspects of function.
In fact, the use of multiple tests is encouraged by the Individuals with Disabilities Education Act (IDEA). Sec. 300.304 states that the public agency must:
- “use a variety of assessment tools and strategies to gather relevant functional, developmental, and academic information about the child”
- “not use any single measure or assessment as the sole criterion for determining whether a child is a child with a disability”
Finally, I commend the investigators for utilizing tests that are functional. They could have chosen laboratory equipment such as balance boards, beams, walking platforms or the like to test balance. In contrast, the balance activities mentioned earlier, such as, reaching, transferring to standing and retrieving items from the floor are activities that students are actually expected to perform in the school. Thus, when utilized at regular intervals on the same student, they are good measures of real functional gains. Since motor learning principles emphasize the specificity of interventions, we should also promote the specificity of tests to outcomes. So, if your goal for the student is to be able to stand up from the chair to retrieve an item within the classroom and go back to his seat, what more appropriate test is out there than one that actually asks the child to get up, walk, turn around and return to his seat?
~~~~~~~~~~ 0 ~~~~~~~~~~
Freakishly Fast Poll
[democracy id=”4″]
Seeking Your Views
What are the challenges you face when utilizing standardized tests in schools?
What standardized tests do you recommend for students who utilize wheelchairs as their primary mode of mobility?
Leave your answers and comments below.
~~~~~~~~~~ 0 ~~~~~~~~~~
Readers of this article also read these:
Top 9 Functional Balance Tests for School-based PTs
Functional Classification Systems for Children with CP
Top 10 Walking Tests for School-based PTs
Motoropoly 4: Motor Learning Principles in School – Motor Imagery & Self-Controlled Practice





2 Pingbacks