Written by Laurie Ray, MPT, PhD, who has over 18 years of experience in school-based practice and is a state-level PT consultant for public schools. She also consults for Medicaid and Adapted Physical Education for her state and is an Associate Professor at UNC-Chapel Hill. Laurie also teaches continuing education via Apply EBP. More about these courses after the article below.
Medicaid, Plan of Care and Documentation 
504, ADA, FERPA & HIPAA 
IEP Decision-Making
[smbtoolbar]
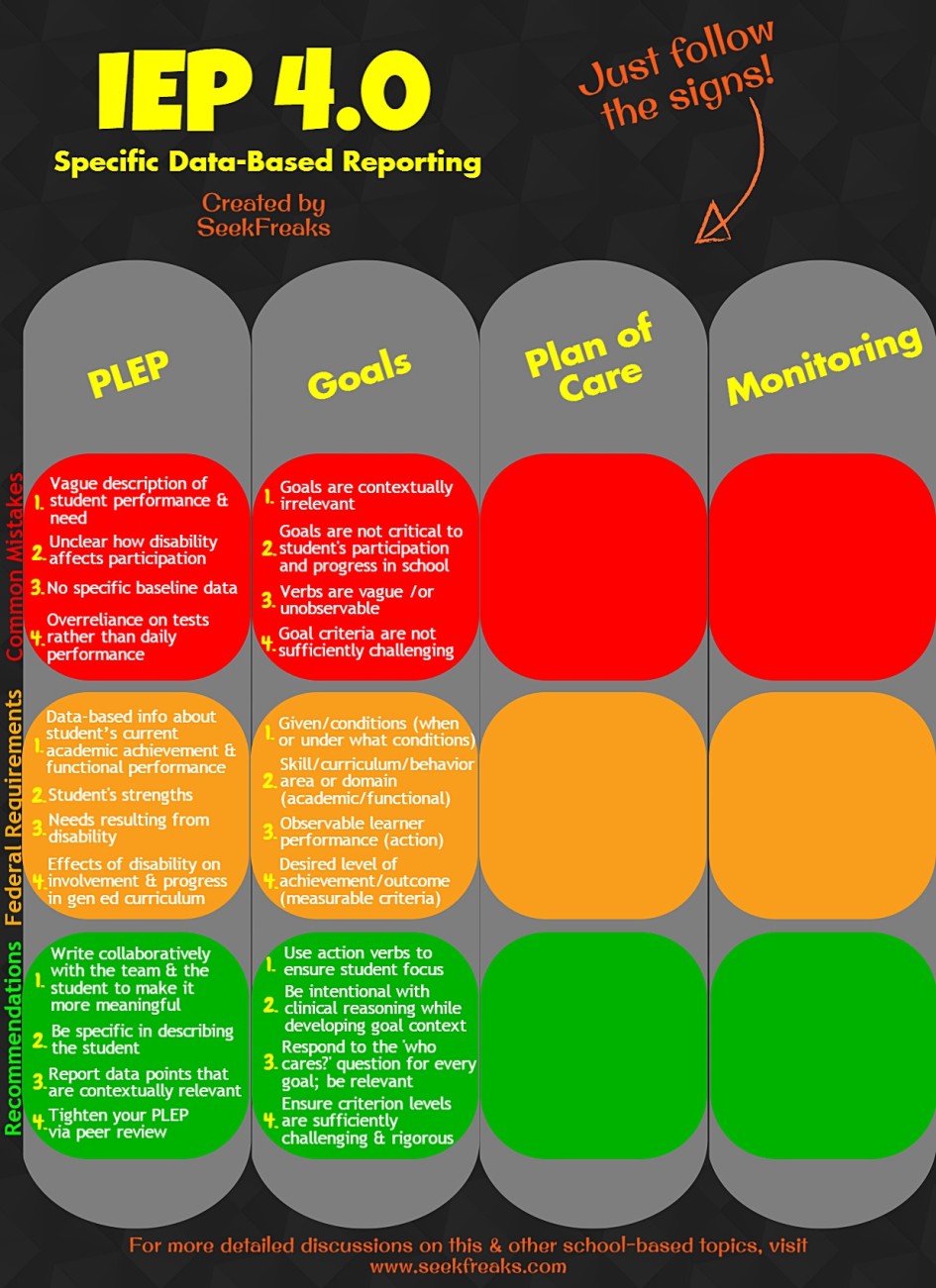
We continue with our IEP 4.0 series to discuss data-based and student-focused goals. In case you missed the first in the series, do read it first by clicking here: IEP 4.0 – Using Data and Collaboration to Develop a Clear PLEP.
Student Goals…how many hours are invested in crafting these guiding lights of our daily work? It is so difficult to peer into the crystal ball and determine how much progress any student will make over the lifetime of the Individual Educational Program (IEP) we are developing. What is the right aspect of the skill? The whole skill? In the hardest context? What specific criterion? Who will measure it? In the SeekFreaks posting last week, Part I, we stated the Present Level of Educational Performance (PLEP) is the cornerstone of the whole IEP. If we have written a PLEP that is rich in data, sufficiently specific and accurate in its assessment/prioritizing of student need, the student goals should be VERY simple to extract. If not, goal writing will be a complicated exercise in forecasting. Please note that I refer to goals as student goals, not annual goals, IEP goals or heaven forfend, PT, OT or Speech goals. I think it is important to keep the student as the focus. The time frame and all other variables can change, but it should be all about student performance.
There seems to be a trend of districts requiring curriculum-based or standards-driven student goals. Is that true in your district? The intent appears to ensure the educational relevance of every goal driving the IEP. Many school-based therapists are intimidated by this and feel that our work is outside of the curriculum, in the daily function of the student. I encourage anyone who feels we operate outside of the curriculum to take the time to examine the part of the curriculum in your state that addresses: health, citizenship, personal choices, identification of health/behavior risks, promotion of healthy, active lifelong behavior, self-determination, among many other essential adult skills needed to enhance a person’s quality of life. Check it out for yourself (project for the summer or a teacher workday?)!! They are often included in physical and health education and are called something similar, like: Physical Development and Health, Health Literacy, 21st Century Skills, Healthful Living, etc. Many things a therapist works on daily with student are included in these standards. Linking our work to the educational standards is not as difficult as it may initially appear.
Given that the PLEP we are drawing goals from is collaborative with the full IEP team (including students and parents in planning especially) and packed with data, writing the student goal should be a snap. During the first IEP cycle when you shift your practice to a more data-based, collaborative approach, more time will be required to communicate and think it out. However, many have told me that, in fact, after the initial change, IEP development takes much less time. AND no one who has shifted his/her practice in this way has told me that they reverted back to developing PLEPs and goals on his/her own, the night before pouring over their notes or prior to the meeting sweating it out over that critical cup of coffee.
A collaborative, data-rich PLEP is less like a snapshot than a carefully wrought portrait. A portrait requires much thought and consideration, featuring the most important focus and speaking a clear message to all who view it. Deriving student goals from such a PLEP, is more like a detail of the portrait than a new work. We are zooming the IEP team’s attention to a specific skill that is so critical to student performance during this IEP that we must commit all our efforts to a student goal.
If student goals are not derived from a data-rich, collaborative IEP, so what?
Top 4 Problems with Student Goals:
- Goals are so clear and specific that they never occur naturally in a school day (e.g. Laurie will stand on one leg for 6 seconds; Laurie will 3 overlapping circles with 100% accuracy). Consequently, no one cares but the PT, OT or Speech services.
- It is not clear why this skill is important to the student’s participation in and progress through the general education curriculum.
- Terms are intentionally vague or unobservable (i.e. using verbs like improve or increase).
- Goal criterion is not sufficiently challenging to progress the student to his/her unknown potential (or risk not achieving the goal).
Usually school-based therapists are ahead of the field with how measurable our goals are. I have heard compliance managers wishing they could get other IEP members to emulate the measurability of goal we develop. BUT we must also ensure that the student goal is critical to education, performance or function. If we are the only one who care about student goals we develop and work on, perhaps the trouble is not ‘buy in’ but that we are not working where the student needs our assistance the most? If no one cares, maybe the problem is not the team but the goal.
Let me take the two example PLEPs from last week and draft some potential goals. I never claim perfect work and welcome you to use the comment section to edit my efforts or rip them to shreds if I got it totally wrong.
Domain= Self-care/Transition
Laurie is a 17-year-old with cerebral palsy that affects her arms and legs (spastic quadriplegic; GMFCS Level V). She has stiffness (extensor hypertonicity) in both her legs and arms (flexor hypertonicity), but her legs are stiffer. Laurie is well positioned in her personal power wheelchair (tilt-in space & postural supports), but doesn’t change positions much during the school day so we worry about her skin breaking down (skin integrity). She is independent with moving throughout her paved campus, can open doors and negotiate crowded hallways. She cannot go to the sports fields as they are inaccessible for her wheelchair. Laurie is dependent on others for and does not initiate/ participate in transfers. She needs moderate physical assistance with activities of daily living including 4-6 verbal cues from staff to adjust wheelchair to table/desk, hygiene (stand by assist with bilateral rails in modified stall and minimal assist doffing clothes/maximum assist with donning clothing) and eating (needs beverages held, stability at elbow and help to load spoon and conduct spoon to mouth). Laurie is very social (attends all dances and social events accessible with public transit) and intelligent; is a rabid ‘texter’. She expresses herself verbally with difficulty, mainly through gestures, facial expressions, saying and nodding “yes” or “no” and pointing with eyes and arms; uses computer/texting for most in depth interactions. Laurie lives with her grandmother who has great difficulty with transfers and struggles with pain. She and her grandmother rely on public transportation and always travel together. Laurie wants to go to college (will take the ACT in September). On the AIR Self-Determination Profile, Laurie is ~60% self-determined (score= 71). This test indicates her capacity for self-determination exceeds her opportunities to be self-determined both at school and home. She plans to take a one class at the community college next semester (need to work out transportation/do accessibility assessment). Laurie has a career goal to be computer programmer or web designer (on the Vocational Rehabilitation waiting list).
- Laurie will lead all transfers and positioning adjustments by counting (1, 2, 3/transfer on 3) for the staff, 2 consecutive school days.
- Laurie will doff clothing independently and don clothing with minimal physical assistance for hygiene needs, 1 full school day.
- Laurie will indicate a need for a position change to staff with a programmed prompt from a device, at least 2 times during the school day.
Transition Goals:
- Laurie, Gigi (grandmother) and team will explore public transit for work sites and community college and develop a workable plan for Laurie to access, independently if possible.
- Laurie will work with her school counselor, OT, PT and job coach to develop work opportunities and a plan for next steps with college and career. This will result in a written plan with timelines and assigned responsibilities.
- Laurie will follow up with Vocational Rehabilitation, given assistance from the job coach and GiGi, to make an appointment for evaluation.
Which part of these goals provide each of the federally required goal components below? Can you improve them better to adhere to these requirements?
| Federally Required Student Goal Component | Laurie’s Goal Statement |
| 1. Given/Conditions (when or under what conditions), as appropriate | |
| 2. Skill/Curriculum/Behavior Area or Domain (Academic/Functional) | |
| 3. Observable Learner Performance (Action) | |
| 4. Desired Level of Achievement/Outcome (Measurable Criteria…how well, how many times, over what period of time) |
Do you think I focused the team efforts on the correct skills? Are there areas ignored that are important with this IEP? Where interventions should take place? Can you see the data needs from various personnel and each disciplines’ role? Could you pinpoint levels of assist for various self-care requirements on a graph as a starting point? Could Laurie participate in data collection? Progress reporting to the IEP team?
Domain= Classroom behaviors/Transitions
Ralph is a 6 year-old boy in 1st grade. He has difficulty sitting on the floor independently for more than 2.5 minutes on average and wants to sit with his legs straight instead of crisscross like his peers or leans on his arms or peers. Ralph can sit upright in his chair for 4 minutes and often leans on his desk/elbows. He stands and sits with poor posture (forward head, rounded shoulders, anterior pelvic tilt, locked knees, low muscle tone and noted joint hypermobility/laxity). Ralph attends to instruction for 3-4 minutes before exhibiting distracting behaviors or repetitive movements. He often lays his head on his desk, sings and talks with peers inappropriately. He can stand from the floor in 11.8 seconds on average (7.5 seconds on average for 5-6yo) and must use his arms. Ralph walks independently in the class, hallway and campus, although slower than peers transitioning between locations (from class to lunchroom/120’ = +2.8 minutes on average). He participates in PE small groups for 7.6 minutes (11.7 average for peers) before sitting down and struggles to participate. Ralph sits and/or talks and does not play or run during recess/free play. Ralph’s parents report having difficulty engaging him in physical activities and limiting his screen time.
- Ralph will sit independently for the full duration of calendar time (4.8 min on average), 3 out of 5 school days. He will not lean on other students, lie down but can prop on his arms and change (leg) position.
- Ralph will play with peers at PE or recess for 9 minutes without resting or stopping, 1 out of 2 daily observations for 3 out of 5 school days.
Let’s try this again! Use the goals above to look for data that answers each of the federally required goal components below. Try to create your own goals that would satisfy these requirements.
| Federally Required Student Goal Component | Ralph’s Goal Statement |
| 1. Given/Conditions (when or under what conditions), as appropriate | |
| 2. Skill/Curriculum/Behavior Area or Domain (Academic/Functional) | |
| 3. Observable Learner Performance (Action) | |
| 4. Desired Level of Achievement/Outcome (Measurable Criteria…how well, how many times, over what period of time) |
Are there other skill areas in the PLEP that can be addressed with these student goals? Where would be your priority for intervention, what time of day or context? Any ideas for home/follow up?
Was the domain/skill area clear? For Laurie, I think increasing self-determination and independence is most critical. Did I miss something that’s key? For Ralph, many other interventions can work to improve these goal areas as well as address other areas of need. Working on play duration will also require endurance, gross motor skills, engagement with peers, strength. If his core strength is sufficient for the independent sitting, I am counting on it also improving his floor to stand times and posture. His greatest area of need seems to be engagement or attention in class/attention to task.
Now get an IEP goal you are working on and use the component chart to find those components in the goal you have. How did you do? Pretty well, I’d guess!! But I hope there are approaches that could be different that you can explore.
What are you thinking about when approaching goals? Employing greater or more intentional clinical reasoning when considering context or criterion? Is this an emerging skill? Am I looking for generalization or consistent mastery? Being specific about time of day or routines? Does the student and IEP team agree this is an area that requires effort, is this change the most important? Every goal we come across can be improved. I again encourage you to utilize the strength of your peers to advance your practice. It is humbling to put forth an unaltered goal for review but it is a fantastic way to identify bad habits, brainstorm creative solutions or occasionally find you are doing great! I look forward to your comments, edits and suggestions!
Continue to Part 3 of IEP 4.0: Collaborative Progress Monitoring
~~~~~~~~~~ 0 ~~~~~~~~~~
References and Resources-
Capizzi, A. M. (2008). From assessment to annual goal: Engaging a decision-making process in writing measurable IEPs. Teaching Exceptional Children, 41(1), 18.
Drasgow, E., Yell, M. L., & Robinson, T. R. (2001). Developing legally correct and educationally appropriate IEPs. Remedial and Special Education, 22(6), 359-373`.
Transition resources: http://transitionta.org/resources
Join author, Laurie Ray, and her colleagues in the following continuing education courses…






March 29, 2016 at 11:07 am
“Setting goals is the first step in turning the invisible into the visible.”
― Tony Robbins
March 29, 2016 at 5:04 pm
I have always looked to improve writing measurable goals. It is a “work in progress”
I have found that working with students on what it is they are interested in is a great place to start 🙂
I would agree that a stop watch is an important tool. 🙂
March 29, 2016 at 11:23 pm
I so agree! Writing student goals is like health management; we can ALWAYS do better…
If the student is interested, that is a great indicator of meaningfulness for the whole team. Do you find that true?
I think the stopwatch makes function measurable. No easier means to monitor progress in my opnion!!⏱❤️
March 29, 2016 at 10:07 pm
You’re so right, Mary Jo, about starting with what the child is interested in. Another reason supporting this is the impact of salience on motor learning, which we will be tackling next week.
May 26, 2016 at 7:12 pm
I have been wearing a stop watch around my neck for years – it is still better than the iPhone for spontaneous measurement: steps, timed distance etc.
August 12, 2016 at 10:49 am
Not only functional but a strong, professional fashion statement Marian!