[smbtoolbar]
I tried telehealth for my own medical care for the first time last month, and was glad to learn it did help, albeit in a different way than if I visited a doctor. There were kinks, including connectivity issues and inability of the doctor to do a physical exam, but there were also advantages. I did not have to go to a doctor when I can barely keep myself in a sitting position, and the doctor seemed genuinely interested in listening to my problems (she was not in a hurry to leave the call). On her end, she was probably also happy to be seeing patients sitting in her home office (an assumption on my part).
Telehealth is here to stay, and perhaps the wave of the future. So we decided to spotlight our colleagues providing telehealth services in school-based practice. We begin with Speech and Language Pathologists who are in the trenches of providing services from their home to anywhere in the US.
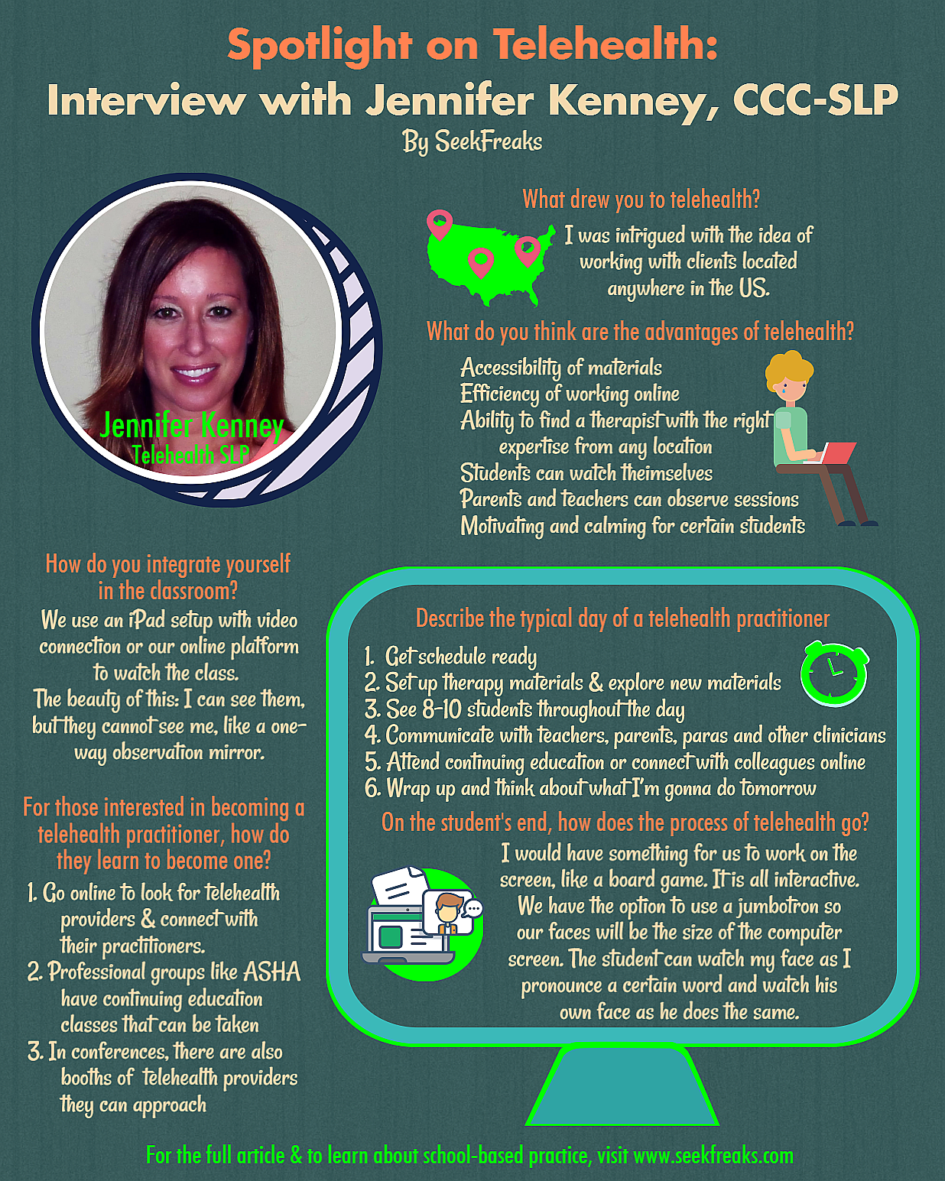
Jennifer Kenney, CCC-SLP, Speech Language Pathologist with Certificate of Clinical Competence (CCC-SLP) practicing for 17 years and in telehealth for the last 5 years, Lead SLP for Presence Learning in San Francisco, CA. She lives in Cary, NC.
~~~~~~~~~~ 0 ~~~~~~~~~~
You are in North Carolina! How long have you been there?
I have been in North Carolina for about 7 years. Prior to that I was in Upstate New York, Saratoga Springs area. I do not miss the cold or the snow for sure.
Did you work in the school system in North Carolina before you became a telehealth practitioner?
I did. I contracted with a few school districts here for about a year and a half. Prior to North Carolina, I was in the public school systems for about 12 years. The school systems down here are large. There’s usually one SLP covering multiple sites. You are traveling a lot, you’re never really consistently in the same building.
What drew you to telehealth?
With that being said, being in the school system, I heard about telehealth and looked into it. This is where the world is going. Everyday there are more and more things happening with technology, right? So, for me, it was a really new idea to think about. I was intrigued with the idea of working with clients located anywhere in the United States. I had a client who lives in Alaska – in Kodiak Island. These students are living in an entirely different culture than in Cary, North Carolina. They go hunting for months out of the school year. They walk to schools in packs to avoid wild animals. This was very intriguing to me.
Other than Alaska, what other states have you covered?
North Carolina, California, and Arizona.
How do you learn their culture, being separate from them?
Not understanding a client’s culture can be a roadblock. The company I work for provides training on culture, about our clients’ daily lives and priorities. Understanding those is an imperative.
Describe a typical day of a telehealth practitioner.
As a clinician, I would start my day getting my schedule, making sure that my therapy materials are all set, exploring new materials. I would then see 8-10 students throughout the day. During my sessions, our online platform already has SOAP notes built in to “my classroom” so I can really be efficient in doing my data collection during my therapy time. At the end of the day, I am just wrapping up and thinking about what I’m going to do tomorrow. In the midst of the day, I’m communicating with teachers, parents, paraprofessionals, and other clinicians in my team. Sometimes, I would attend continuing education, or hangout on Yammer, our social media platform, to find out what’s happening with other telehealth practitioners across the country. Yammer is like Facebook, but closed. People will be on there posting pictures, or posing questions about their clients. It is for social purposes and collaboration, as well.
What’s your typical set up at home?
My computer (LOL). That’s about it. And I move around the house for different sceneries. All of our materials are built into our online system. We have hundreds of thousands of activities, based on age, grade, specific areas of function. For example, you can find activities for students learning the S sound, by entering a search like on Google. There are new things on it everyday that clinicians upload. If each of the 700 clinicians upload an activity a day, imagine how many activities can be on there. We all share materials.
On the student’s end, how does the process of telehealth go?
We work a schedule with the teacher, paraprofessional or administrator. When therapy is scheduled, the school contact, for example, a paraprofessional, would bring the student from class to a computer and sign them on. The “doorbell” in my room would ring, and we turn on the camera, and we go!
I would have something for us to work on the screen, for example, a board game. It is all interactive, so if we pick stamps as our topic, our game board, we are spinning spinners, and we are moving pieces across the gameboard on the screen. We can see what each of us are doing with our pieces on the screen. If we are using a deck of cards for speech sounds, we go from card to card.

Screenshot of telehealth SLP online platform (copyright of PresenceLearning; used with permission)
Whatever their IEP goal is, that’s what I am targeting with them. Within that therapy session, we will be working together. We have the option to use a jumbotron so our faces will be the size of the computer screen, where we will look like we are sitting next to each other. Our students can watch my face as I pronounce a certain word and watch his own face as he does the same.
The neat thing about it – how often in a typical day do you see yourself when you are engaging with somebody? You don’t! You never know what you look like when you are talking This is a cool thing, because if a student is learning to make a certain sound, they can see their mouth, what they are doing. When normally, you can’t do that.
What improvements would you like to see with telehealth?
I would hope to see telehealth continuing to stay up to date with technology and the ever-so changing world we live in. Also, continuing to explore and improve assessments in order to determine service needs.
What do you think are the advantages of telehealth over face-to-face services?
It’s hard to narrow it down to one. The accessibility of materials and the efficiency of working online is probably the biggest benefit. The other benefit to myself and a client: if a student requires a certain expertise or speaks a very specific language, we are able to find a therapist somewhere who can potentially work with the student. How often can you find what you need in one location?
What are the obstacles for telehealth practitioners?
Obviously, you cannot be hands-on with the child. You cannot manipulate their mouth, or put your hand on their arm to get their attention. The way I have dealt with this is by developing good rapport with the paraprofessional and I have them assist.
How do you integrate yourself in the classroom?
Back in Alaska, we had a student who needed assistance and they wanted me to observe the students in class. We incorporated an irobot, which is basically an iPad setup with video connection, and they would “stick” me in the classroom. Or we can also do this via our online platform. The beauty of our platform – something you can’t do when you are in the school – I have the ability to turn off my camera. So I can see them but they cannot see me, just like in a one-way observation mirror. (In the same way, I can even have a parent or teacher log on to the platform and watch the child without the child knowing the parent is there.)
How do you make sure what you are teaching is related to what’s happening in the classroom?
I communicate with the teachers and staff regularly. I typically email them about what happened in the session that was just completed. In the same way, teachers and staff emails me when they have a concern.
Do you provide group sessions?
Yes, 2 students is typically the max for a computer. Or you can use 2 computers with 2 students each for a maximum of 4 students. It is hard to put more than that. But I can then interact with multiple students.
Do you miss being in the classroom?
That’s a really good question. It’s a hard question to answer because I do not want to say no, because that may not sound like I did not enjoy working face-to-face with a child. But I know that I will be sticking with telehealth. There is so much aspect of it that is now part of my practice. I have a great community and do collaborate with my online colleagues and team. I feel like what I’m doing now is more efficient and motivating to students. They love technology, there is so much that I can do with them, that I may not be able to do if I work with them face-to-face.
Describe how you see that the students are motivated. Why do you think they are motivated?
I think it is just the generation of kids who grew up with technology. The students don’t realize that they are working. They are having a great time. It is very different from being in the classroom. It is so much more interactive – there are animations and videos. And I am able to tailor the session to their needs.

Telehealth SLP session (copyright of PresenceLearning; used with permission)
The autism and social pragmatic piece is very much needed right now. My personal experience is that face-to-face, these students get anxious going into that room with this lady. In telehealth, they are not as anxious on the computer, because the other lady is not sitting right next to them. It is somebody on the computer screen. So I find that I am able to engage them so much more.
And for children with ADHD, ADD, I find the actual screen can be calming for them. I heard people tell me, I don’t know if the student is going to do so well, as he has autism, social communication problems – they are the ones that typically end up enjoying the sessions the most. I’ve also had great success with children with apraxia and motor planning problem. They can see the motion of their mouths without putting a mirror in front of them. So telehealth have been really helpful for these children too.
If you can do a 30-second elevator pitch to convince parents that telehealth works, what would you say?
The accessibility of a therapist who can address the child’s need; the accessibility for parents and teachers to observe what’s going on, as that really helps with carryover and collaboration. We know that therapy does not work with 30 minute sessions a week. It works with the 30-minute session plus the carryover, and the education and collaboration with other staff to make sure the student succeed in their school life.
If somebody is thinking right now about becoming a telehealth practitioner, what should do? How do they learn to become one?
Go online to look for telehealth providers and connect with their practitioners. Watch telehealth videos online. Telehealth providers typically have sample videos on their websites. ASHA too has continuing education classes that can be taken (and I’m sure other organizations, such as the APTA and AOTA do too). ASHA has been backing up the validity of the practice for over 10 years now. In conferences, there are also booths of telehealth providers that you can approach.
~~~~~~~~~~ 0 ~~~~~~~~~~
What do you think, SeekFreaks? Interesting? Promising?
~~~~~~~~~~ 0 ~~~~~~~~~~
Readers of this article also read: